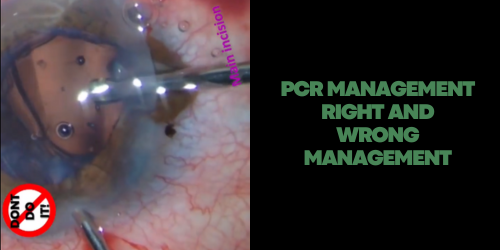
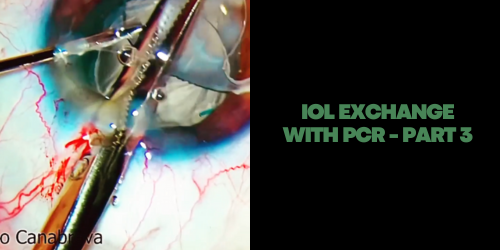
In PCR we recommend pars plana vitrectomy or to create New Small Incision in the Cornea. In this management is essential:
– Don’t use the main incision.
– The vitrectomy through the main incision tends to lose more vitreous. – The use of triamcinolone to better vitreous visualization, making the anterior vitrectomy more effective.
– A scleral incision should be created 3.0 – 3.5 mm posterior to the limbus to access the vitreous behind in pars plana vitrectomy.
– The vitreophagus tip is used in maximum cutter.
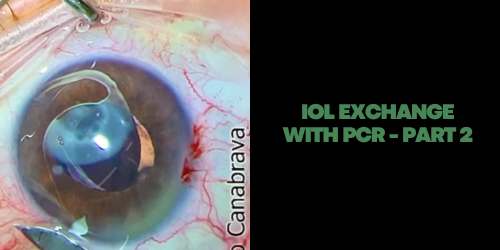
– There are two modes to set the vitrectomy. The “Cutting – I/A” and the “I /A – Cutting”. The first one is indicated for the vitrectomy, because the machine “cut” the vitreous first. The second one is indicated after the vitrectomy has been performed. The rule is to set to the highest speed cutter, however, the aspiration, intraocular pressure, and vacuum must be set to lower limits. – Once the vitreous has been removed from the anterior chamber and the incisions, the next step is to switch to the I/A Cutting mode to remove the remaining cortex.
– The vitrectomy through the main incision tends to lose more vitreous – Parameters: 23G tip: Bottle height: 75cm / Vacuum: 150-200mmHg / Flow rate: 10-15cc/min / Cutting: maximum.