PROLAPSE OF THE IRIS
– Step 1: decrease the pressure of the anterior chamber
– Step 2: iris spatula by the side incision

PROLAPSE OF THE IRIS
– Step 1: decrease the pressure of the anterior chamber
– Step 2: iris spatula by the side incision

ACUTE MISDIRECTION SYNDROME
Characterized: anterior chamber very shallow, with absence of supracoroidian effusion or hemorrhage and without perceptible pathology in iris-lens diaphragm. It usually relieves phacoemulsification without intercurrences in hypermetropic eyes. Pathophysiology: Inadequate movement of balanced saline solution (BSS) through the zonular fibers that accumulate, therefore in the posterior segment generating an increase in posterior pressure, resulting in anterior displacement of the iris-lens diaphragm, axial and anterior peripheral chamber flattening and secondary angular closure. It is normally occurred in the end of the phacoemulsification. Facing such situations, pars plana decompression is necessary, but one should first be sure that there is no evidence of choroidal effusion or bleeding.
Decompression may be done by puncture with a straight 26G insulin needle 3 mm from the limbus followed by aspiration of the fluid posterior to the bag or using a vitrectomy trocater (caliber 23, 25 or 27) to remove retrocapsular fluid using a high shear rate.

CANABRAVA RING by AJL OPHTHALMIC/SPAIN – Start to develop the technique in eyes with pupil between 3.5 – 4 mm, White-White diameter > 10.5 mm and long eyes. It is important to start
THE RING
It is a PMMA ring with a 60º semi-arch opening, internal diameter of 6.3mm and a vertical length of 0.4mm. Its technology differs from competing pupil expansion devices because the parts that attach to the iris (indents) are arranged in an alternating fashion. There are 7 indents (0.9 mm horizontal length), which are positioned in the ring in an alternating manner – one facing upwards and the next downwards.
These alternating attachments are horizontally, but not vertically, aligned. They are specifically spaced from each other to create sufficient room when arranged in the iris. There are 2 small hooks at each end, which attach to the iris. Each indent has a 0.28 mm-wide orifice for intraocular device manipulation with a Sinskey hook. CR is the first pupil ring to have indents that do not superiorly and inferiorly align with each other, resulting in a reduced vertical ring length. It attaches to the iris in a corrugated manner between superior and inferior indents, thus allowing for superior fixation to the pupil border using the narrowest width possible for a PMMA ring. The ring’s compact layout minimizes its thickness, ensuring it easily enters the ocular globe. This makes implantation easier as the iris connects to the ring like a wave.
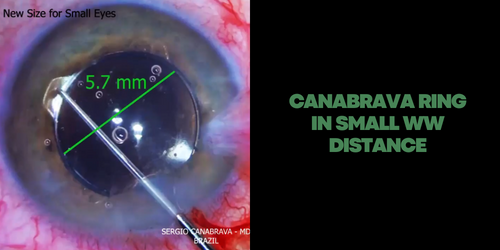
NEW TESTS FOR SMALL EYES!! Here the first test with 5.7 mm CANABRAVA RING! The traditional one has 6.3 mm! You don’t believe how this 0.6 mm are important in eyes with WTW smaller than 10.5 mm. In my experience, I don’t suggest the use off any Iris Expansion Ring with 6.3 mm for eyes with WTW smaller than 10.5 mm!
Notice how the ring is stable during the surgery!
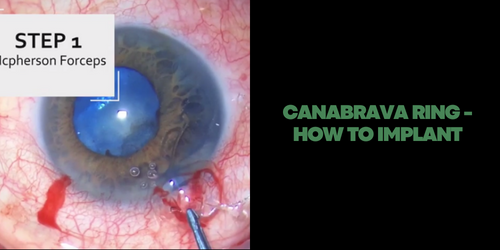
CANABRAVA RING – STEPS TO INSERT
Step 1: McPherson Forceps were used to insert the first half of the ring into the eye, and then, the other half was rotated into the eye using a Sinskey Hook
Step 2: The small central inferior indent was then inserted beneath the iris
Step 3: This process was repeated for each inferior indent
Step 4: The insertion of the CR was completed by docking its hooks below the iris via connection of the Sinskey Hook to the superior indents.

Thanks @seguemed for this amazing device to make easy the Canabrava Technique!! Available to by with Seguemed!
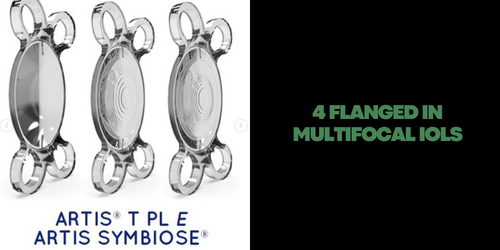
MULTIFOCAL IOL + Canabrava 4-Flanged Technique! Is it possible? YES!!
Dr. Sohee Jeon @averyplantglass (Keye Eye Center, Seoul, Republic of Korea) describeb two cases of premium IOL (toric and multifocal) implantation after which the patients fully recovered their visual function following a Canabrava Four Flanged technique via a 2.8-mm corneal incision. She used Artis IOL Cristalens – France.
Full paper on American Journal of Case Reports.
Congratulations Dr Sohee Jeon! The paper, the surgery and the results are amazing!
* Be careful. Dr. Jeon is an expert surgeon and has many exams to help her in centering the IOL. Do not try to do this before much practice.
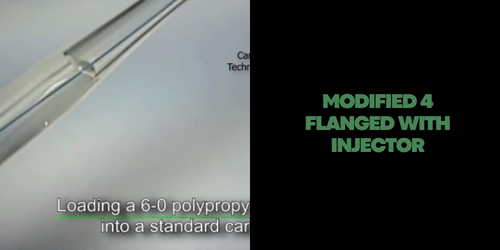
Dr. Mahler from Israel was faster than the Inventor to publish the technique with injector!
Here a great modification in the IOL injection by cartridge by Dr. Ori Mahler
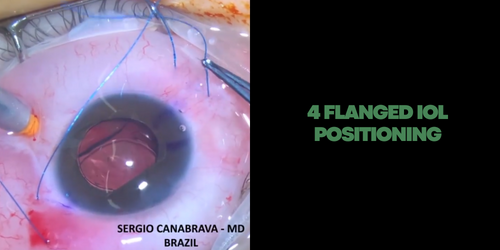
One of the advantages of the technique is that you can easily position the IOL using the 4 adjustable sutures. I am honored to have opened, in 2017, this new way in cataract surgery and watch many great surgeons around the world using my double flanged polypropylene concept to develop new techniques and help patients!!
Attention: never forget to bury the flanges