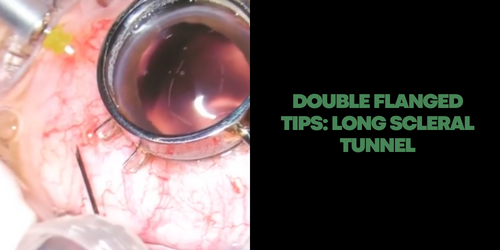
OUBLE FLANGED – Basic Principles #4: Go for a long scleral tunnel
Never insert the needle directly in the sclera! It is import to create a long scleral tunnel to bury the flanged and avoid endophthalmithis!
OUBLE FLANGED – Basic Principles #4: Go for a long scleral tunnel
Never insert the needle directly in the sclera! It is import to create a long scleral tunnel to bury the flanged and avoid endophthalmithis!
Since I first published the Double Flanged technique in 2017, it becomes popular around the world. However, I have seen many surgeons doing the technique differently than the one published. This can bring complications like endophthalmitis, conjunctival erosion and externalized flanged. In order to reduce these complications and to help surgeons starting in the technique. We produced this video with the 10 basic principles of the technique
1 – Material needed
2 – Test the polypropylene before inserting it into the eye
3 – Set up a 2 mm entry point from the limbus
4 – Go for a long scleral tunnel
5 – Push the prolene into the eye while to remove the needle
6 – Hold the base of the prolene with tension
7 – Cut the prolene at the 1,2 to 1,5 mm to the sclera
8 – Flange size
9 – Bury the flanged prolene into the sclera
10 – Be careful piercing IOLs
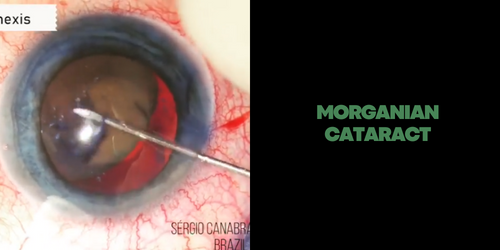
MORGANAGNIAN + BAG FLAGILITY
Important in this case – Notice the bag above the iris during the CTR implantation
– Bag replacement with hook
– Optic capture

HARADA UVEITIS + SMALL PUPIL
Preoperative Conduct:
1- Uveitis Inactivity Period: At least three months.
2- Preoperative oral corticoid: 1mg / kg between 7 and 10 days before surgery.
3 – IOL Implant: do not implant in patients with juvenile rheumatoid arthritis. It is possible to implant in others uveitis
Intraoperative Conduct:
1- Small Pupil Strategy: Preference for pupil expansion ring. Iris retractors causes greater trauma and need to make 4 additional paracentesis openings.
2- Anterior synechiae: Always the first step that must be accomplished. It decreases the risk of corneal decompensation during surgery. We recommend using an iris spatula.
3- Intraoperative Iridectomy: Performed routinely. Prevent postoperative inflammatory pupillary block.
Postoperative Conduct:
1- Corticosteroid Reduction: 0.1mg / kg / week
2- Medical Returns: These should be frequent, often occurring daily in the first week for monitoring inflammation and intraocular pressure.
Handling always performed by the cataract department and the uveitis department together.
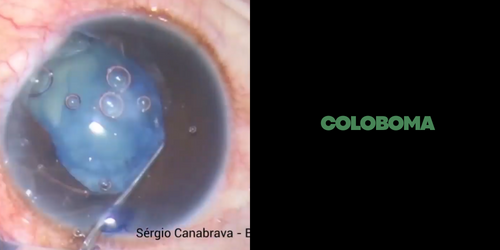
IRIS COLOBOMA + CANABRAVA RING + CTR + PUPILLOPLASTY
Today, the part II
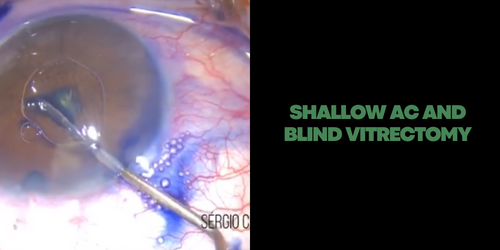
Extreme shallow anterior chamber + Vitrectomy
Observe how the anterior chamber was extreme shallow before to performed a blind descompression vitrectomy. The Canabrava ring is a good option in this kind of case because it has 0.4 mm height and Malyugin, Oasys and I-ring has 0.8 mm height. And please, iris hook in this kind of patient is a suicide!!!
Observe how fragile the zonule is. I inserted the 10/12 mm CTR inside the bag before the phaco and hidroprolapsed the nucleus to the anterior chamber. After removing the cortex….PCR.
The Double Flanged Polypropylene Suture open many techniques! Here one interesting.
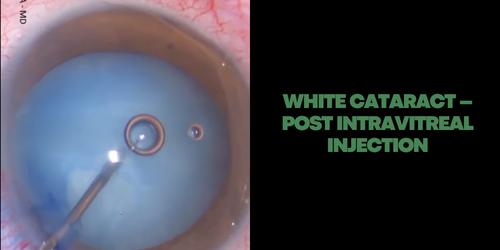
Here the answer why “Tilt and tumble” technique posted last week! I don’t suggest Phacoemulsification inside the bag in post Bevacizumab cataract! You never knows about posterior capsule integrity’s!
It always a challenging.. my advice is.. always go slowly